Radiation is all around us. We are continually exposed to natural background radiation and it seems to be without any problem. Yes, high doses of ionizing radiation is harmful and potentially lethal to living beings, but these doses must be really high. Moreover, what is not harmful in high doses? Even high amount of water can be lethal to living beings.
The truth about low-dose radiation health effects still needs to be found. It is not exactly known, whether these low doses of radiation are detrimental or beneficial (and where is the threshold). There are studies, that claim, that small doses of radiation given at a low dose rate stimulate the defense mechanisms. Moreover, ionizing radiation can have health benefits in medicine, for example, in diagnostics where X-rays are used to produce pictures of the inside of the body. We do not claim, everything is OK. It also depends on the type of radiation and tissue, which was exposed.
But finally, if you compare risks, which arise from existence of radiation, natural or artificial, with risks, which arise from everyday life, then you must conclude that fear of radiation is irrational. Humans are often inconsistent in our treatment of perceived risks. Even though two situations may have similar risks, people will find one situation permissible and another unjustifiably dangerous.
The problem of ionizing radiation lies in the fact that the radiation is invisible and not directly detectable by human senses. People can neither see nor feel radiation, and therefore they feel fear of this invisible threat.

How Dangerous is Radiation
Radiation is all around us. In, around, and above the world we live in. It is a natural energy force that surrounds us. It is a part of our natural world that has been here since the birth of our planet. All living creatures, from the beginning of time, have been, and are still being, exposed to ionizing radiation.
For example, potassium-40 is one of isotopes which contributes to internal exposure of human. Traces of potassium-40 are found in all potassium, and it is the most common radioisotope in the human body. Higher amounts can be also found in bananas. Does it mean, eating bananas must be dangerous? Of course not.
Whether the source of radiation is natural or man-made, whether it is a large dose of radiation or a small dose, there will be some biological effects. In general, ionizing radiation is harmful and potentially lethal to living beings but can have health benefits in medicine, for example, in radiation therapy for the treatment of cancer and thyrotoxicosis.
In the following thoughts, we try to summarize facts and hypothesis, which can help you understand the problem. It is all about the risks arising from exposure to ionizing radiation and about the consistency in all risks of everyday life. But first we have to summarize key facts about ionizing radiation.
Intensity of Radiation – Dose and Dose Rate
Intensity of ionizing radiation is a key factor, which determines health effects from being exposed to any radiation. It is similar as being exposed to heat radiation from a fire (in fact, it is also transferred by photons). If you are too close to a fire, the intensity of thermal radiation is high and you can get burned. If you are at the right distance, you can withstand there without any problems and moreover it is comfortable. If you are too far from heat source, the insufficiency of heat can also hurt you. This analogy, in a certain sense, can be applied to radiation also from ionizing radiation sources.
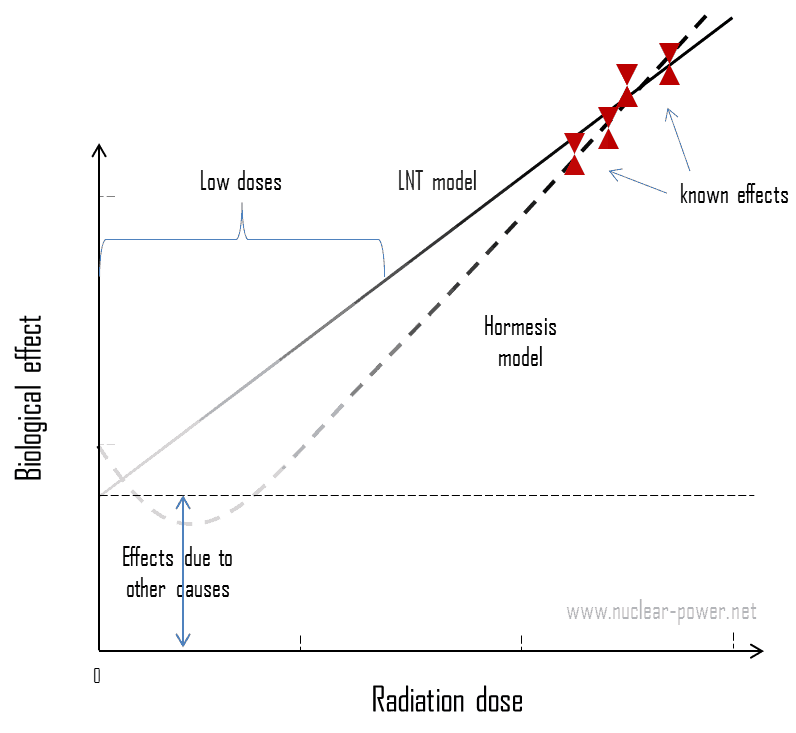
In short, to get burned (deterministic effects and demonstrable stochastic effects) by ionizing radiation, you must be exposed to really high amount of radiation. But almost everytime, we are talking about so called low doses. As was written, today the protection system is based on the LNT-hypothesis, which is a conservative model used in radiation protection to estimate the health effects from small radiation doses. This model is excellent for setting up a protection system for all use of ionizing radiation. This model assumes, that there is no threshold point and risk increases linearly with a dose, i.e. the LNT model implies that there is no safe dose of ionizing radiation. If this linear model is correct, then natural background radiation is the most hazardous source of radiation to general public health, followed by medical imaging as a close second. It must be added, the research during the last two decades is very interesting and show that small doses of radiation given at a low dose rate stimulate the defense mechanisms. Therefore the LNT model is not universally accepted with some proposing an adaptive dose–response relationship where low doses are protective and high doses are detrimental. Many studies have contradicted the LNT model and many of these have shown adaptive response to low dose radiation resulting in reduced mutations and cancers. On the other hand, it is very important, to what type of radiation is a person exposed.
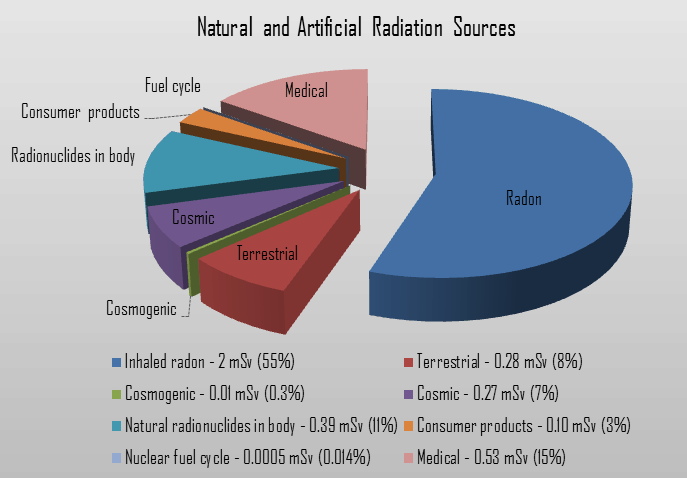 Natural background radiation is ionizing radiation, that originates from a variety of natural sources. All living creatures, from the beginning of time, have been, and are still being, exposed to ionizing radiation. This radiation is not associated with any human activity. There are radioactive isotopes in our bodies, houses, air, water and in the soil. We all are also exposed to radiation from outer space.
Natural background radiation is ionizing radiation, that originates from a variety of natural sources. All living creatures, from the beginning of time, have been, and are still being, exposed to ionizing radiation. This radiation is not associated with any human activity. There are radioactive isotopes in our bodies, houses, air, water and in the soil. We all are also exposed to radiation from outer space.
Sources of Natural Background Radiation
We divide all these natural radiation sources into three groups:
You can not go through life without radiation. The danger of ionizing radiation lies in the fact that the radiation is invisible and not directly detectable by human senses. People can neither see nor feel radiation, yet it deposits energy to the molecules of the body.
But don’t worry, the doses from background radiation are usually very small (except radon exposure). Low dose here means additional small doses comparable to the normal background radiation (10 µSv = average daily dose received from natural background). The problem is that, at very low doses, it is practically impossible to correlate any irradiation with certain biological effects. This is because the baseline cancer rate is already very high and the risk of developing cancer fluctuates 40% because of individual life style and environmental effects, obscuring the subtle effects of low-level radiation.
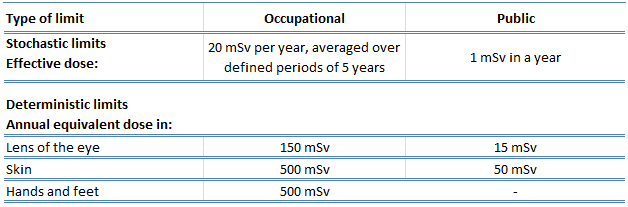
In radiation protection, dose limits are set to limit stochastic effects to an acceptable level, and to prevent deterministic effects completely. Note that, stochastic effects are those arising from chance: the greater the dose, the more likely the effect. Deterministic effects are those which normally have a threshold: above this, the severity of the effect increases with the dose. Dose limits are a fundamental component of radiation protection, and breaching these limits is against radiation regulation in most countries. Note that, the dose limits described in this article apply to routine operations. They do not apply to an emergency situation when human life is endangered. They do not apply in emergency exposure situations where an individual is attempting to prevent a catastrophic situation.
The limits are split into two groups, the public, and occupationally exposed workers. According to ICRP, occupational exposure refers to all exposure incurred by workers in the course of their work, with the exception of
- excluded exposures and exposures from exempt activities involving radiation or exempt sources
- any medical exposure
- the normal local natural background radiation.
The following table summarizes dose limits for occupationally exposed workers and for the public:
Source of data: ICRP, 2007. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 37 (2-4).
Source of data: ICRP, 2007. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 37 (2-4).
According to the recommendation of the ICRP in its statement on tissue reactions of 21. April 2011, the equivalent dose limit for the lens of the eye for occupational exposure in planned exposure situations was reduced from 150 mSv/year to 20 mSv/year, averaged over defined periods of 5 years, with no annual dose in a single year exceeding 50 mSv.
Limits on effective dose are for the sum of the relevant effective doses from external exposure in the specified time period and the committed effective dose from intakes of radionuclides in the same period. For adults, the committed effective dose is computed for a 50-year period after intake, whereas for children it is computed for the period up to age 70 years. The effective whole-body dose limit of 20 mSv is an average value over five years. The real limit is 100 mSv in 5 years, with not more than 50 mSv in any one year.
Type of Radiation – High-LET x Low-LET
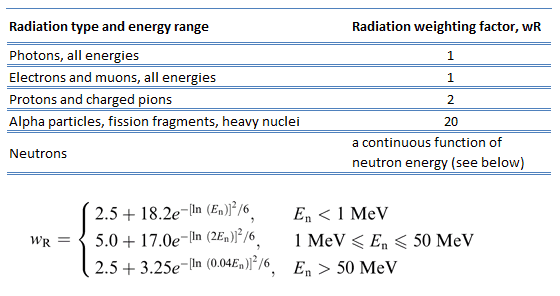
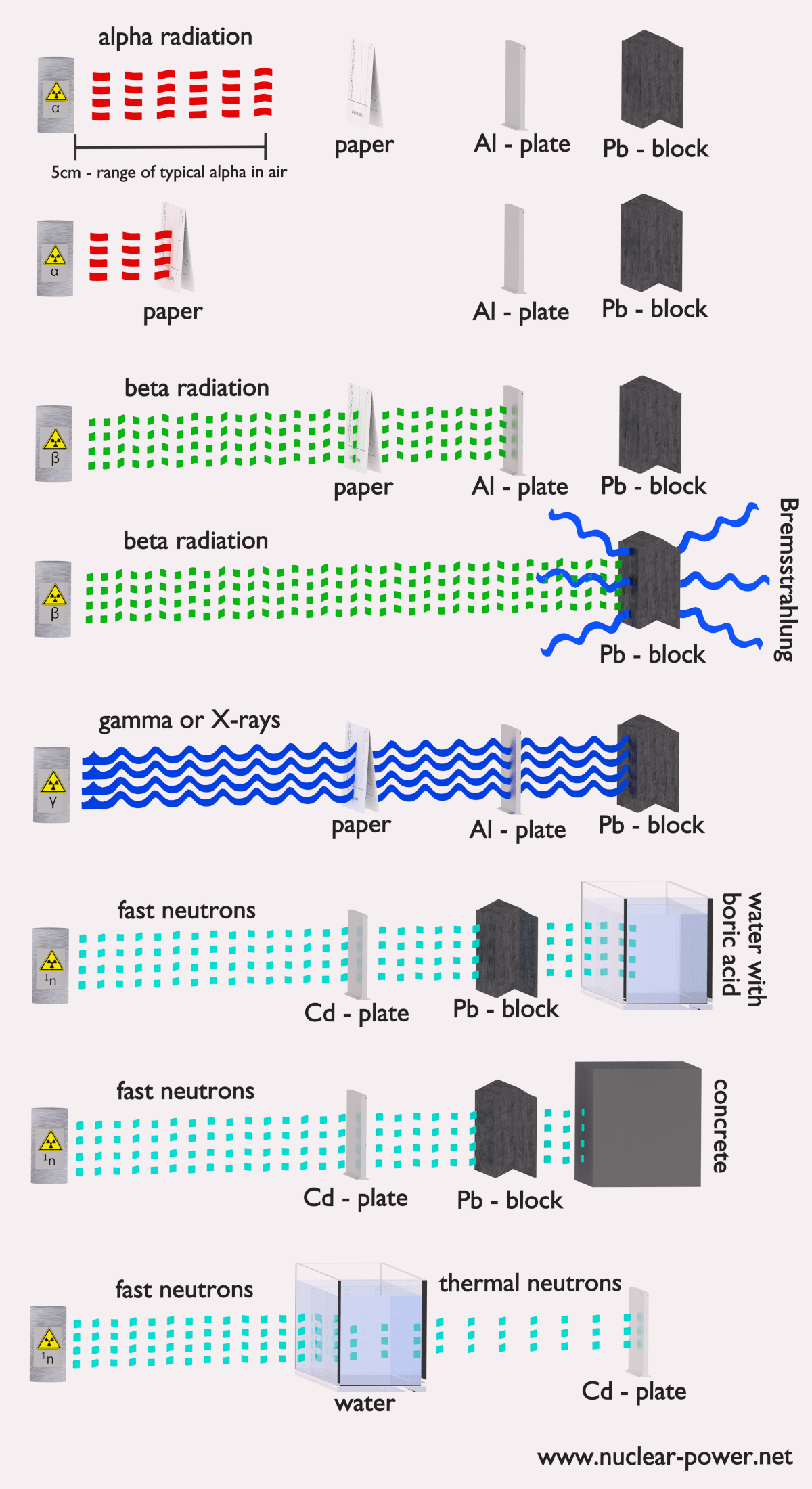
This section is about the fact, that there are several types of ionizing radiation and each type of radiation interacts with matter in a different way. When discussing the intensity of radiation, we have to take into account to which type of radiation are you exposed. For example, alpha radiation tend to travel only a short distance and do not penetrate very far into tissue if at all. Therefore, alpha radiation is sometimes treated as non-hazardous, since it cannot penetrate surface layers of human skin. This is naturally true, but this is not valid for internal exposure by alpha radionuclides. When inhaled or ingested, alpha radiation is much more dangerous than other types of radiation. Note that, the radiation weighting factor for alpha radiation is equal to 20. It was discovered, biological effects of any radiation increases with the linear energy transfer (LET). In short, the biological damage from high-LET radiation (alpha particles, protons or neutrons) is much greater than that from low-LET radiation (gamma rays).
 Ionizing radiation is categorized by the nature of the particles or electromagnetic waves that create the ionizing effect. These particles/waves have different ionization mechanisms, and may be grouped as:
Ionizing radiation is categorized by the nature of the particles or electromagnetic waves that create the ionizing effect. These particles/waves have different ionization mechanisms, and may be grouped as:
- Directly ionizing. Charged particles (atomic nuclei, electrons, positrons, protons, muons, etc.) can ionize atoms directly by fundamental interaction through the Coulomb force if it carries sufficient kinetic energy. These particles must be moving at relativistic speeds to reach the required kinetic energy. Even photons (gamma rays and X-rays) can ionize atoms directly (despite they are electrically neutral) through the Photoelectric effect and the Compton effect, but secondary (indirect) ionization is much more significant.
- Indirectly ionizing. Indirect ionizing radiation is electrically neutral particles and therefore does not interact strongly with matter. The bulk of the ionization effects are due to secondary ionizations.
External x Internal Exposure
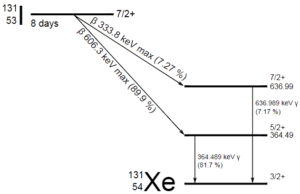
As was written, it is crucial, whether we are exposed to radiation from external sources or from internal sources. This is similar as for another dangerous substances. Internal exposure is more dangerous than external exposure, since we are carrying the source of radiation inside our bodies and we cannot use any of radiation protection principles (time, distance, shielding). The intake of radioactive material can occur through various pathways such as ingestion of radioactive contamination in food or liquids, inhalation of radioactive gases, or through intact or wounded skin. On this place, we have to distinguish between radiation and contamination. Radioactive contamination consist of radioactive material, that generate ionizing radiation. It is the source of radiation, not radiation itself. Anytime that radioactive material is not in a sealed radioactive source container and might be spread onto other objects, radioactive contamination is a possibility. For example, radioiodine, iodine-131, is an important radioisotope of iodine. Radioiodine plays a major role as a radioactive isotope present in nuclear fission products, and it is a major contributor to the health hazards when released into the atmosphere during an accident. Iodine-131 has a half-life of 8.02 days. The target tissue for radioiodine exposure is the thyroid gland. The external beta and gamma dose from radioiodine present in the air is quite negligible when compared to the committed dose to the thyroid that would result from breathing this air.
If the source of radiation is inside our body, we say, it is internal exposure. The intake of radioactive material can occur through various pathways such as ingestion of radioactive contamination in food or liquids, inhalation of radioactive gases, or through intact or wounded skin. Most radionuclides will give you much more radiation dose if they can somehow enter your body, than they would if they remained outside. For internal doses, we first should distinguish between intake and uptake. Intake means what a person takes in. Uptake means what a person keeps.
When a radioactive compound enters the body, the activity will decrease with time, due both to radioactive decay and to biological clearance. The decrease varies from one radioactive compound to another. For this purpose, the biological half-life is defined in radiation protection.
The biological half-life is the time taken for the amount of a particular element in the body to decrease to half of its initial value due to elimination by biological processes alone, when the rate of removal is roughly exponential. The biological half-life depends on the rate at which the body normally uses a particular compound of an element. Radioactive isotopes that were ingested or taken in through other pathways will gradually be removed from the body via bowels, kidneys, respiration and perspiration. This means that a radioactive substance can be expelled before it has had the chance to decay.
As a result, the biological half-life significantly influences the effective half-life and the overall dose from internal contamination. If a radioactive compound with radioactive half-life (t1/2) is cleared from the body with a biological half-life tb, the effective half-life (te) is given by the expression:
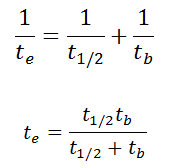
As can be seen, the biological mechanisms always decreases the overall dose from internal contamination. Moreover, if t1/2 is large in comparison to tb, the effective half-life is approximately the same as tb.
For example, tritium has the biological half-life about 10 days, while the radioactive half-life is about 12 years. On the other hand, radionuclides with very short radioactive half-lives have also very short effective half-lives. These radionuclides will deliver, for all practical purposes, the total radiation dose within the first few days or weeks after intake.
For tritium, the annual limit intake (ALI) is 1 x 109 Bq. If you take in 1 x 109 Bq of tritium, you will receive a whole-body dose of 20 mSv. The committed effective dose, E(t), is therefore 20 mSv. It does not depend whether a person intakes this amount of activity in a short time or in a long time. In every case, this person gets the same whole-body dose of 20 mSv.
Airborne contamination is of particular importance in nuclear power plants, where it must be monitored. Contaminants can become airborne especially during reactor top head remove, reactor refueling, and during manipulations within spent fuel pool. The air can be contaminated with radioactive isotopes especially in particulate form, which poses a particular inhalation hazard. This contamination consists of various fission and activation products that enter the air in gaseous, vapour or particulate form. There are four types of airborne contamination in nuclear power plants, namely:
- Particulates. Particulate activity is an internal hazard, because it can be inhaled. Transportable particulate material taken into the respiratory system will enter the blood stream and be carried to all parts of the body. Non-transportable particulates will stay in the lungs with a certain biological half-life. For example, Sr-90, Ra-226 and Pu-239 are radionuclides known as bone-seeking radionuclides. These radionuclides have long biological half-lives and are serious internal hazards. Once deposited in bone, they remain there essentially unchanged in amount during the lifetime of the individual. The continued action of the emitted alpha particles can cause significant injury: over many years they deposit all their energy in a tiny volume of tissue, because the range of the alpha particles is very short.
- Noble gases. Radioactive noble gases, such as xenon-133, xenon-135 and krypton-85 are present in reactor coolant especially when fuel leakages are present. As they appear in coolant, they become airborne and they can be inhaled. They are exhaled right after they are inhaled, because the body does not react chemically with them. If workers are working in a noble gas cloud, the external dose they will receive is about 1000 times greater than the internal dose. Because of this, we are only concerned about the external beta and gamma dose rates.
 Radioiodine. Radioiodine, iodine-131, is an important radioisotope of iodine. Radioiodine plays a major role as a radioactive isotope present in nuclear fission products, and it is a major contributor to the health hazards when released into the atmosphere during an accident. Iodine-131 has a half-life of 8.02 days. The target tissue for radioiodine exposure is the thyroid gland. The external beta and gamma dose from radioiodine present in the air is quite negligible when compared to the committed dose to the thyroid that would result from breathing this air. The biological half-life for iodine inside the human body is about 80 days (according to ICRP). Iodine in food is absorbed by the body and preferentially concentrated in the thyroid where it is needed for the functioning of that gland. When 131I is present in high levels in the environment from radioactive fallout, it can be absorbed through contaminated food, and will also accumulate in the thyroid. 131I decays with a half-life of 8.02 days with beta particle and gamma emissions. As it decays, it may cause damage to the thyroid. The primary risk from exposure to high levels of 131I is the chance occurrence of radiogenic thyroid cancer in later life. For 131I, ICRP has calculated that if you inhale 1 x 106 Bq, you will receive a thyroid dose of HT = 400 mSv (and weighted whole-body dose of 20 mSv).
Radioiodine. Radioiodine, iodine-131, is an important radioisotope of iodine. Radioiodine plays a major role as a radioactive isotope present in nuclear fission products, and it is a major contributor to the health hazards when released into the atmosphere during an accident. Iodine-131 has a half-life of 8.02 days. The target tissue for radioiodine exposure is the thyroid gland. The external beta and gamma dose from radioiodine present in the air is quite negligible when compared to the committed dose to the thyroid that would result from breathing this air. The biological half-life for iodine inside the human body is about 80 days (according to ICRP). Iodine in food is absorbed by the body and preferentially concentrated in the thyroid where it is needed for the functioning of that gland. When 131I is present in high levels in the environment from radioactive fallout, it can be absorbed through contaminated food, and will also accumulate in the thyroid. 131I decays with a half-life of 8.02 days with beta particle and gamma emissions. As it decays, it may cause damage to the thyroid. The primary risk from exposure to high levels of 131I is the chance occurrence of radiogenic thyroid cancer in later life. For 131I, ICRP has calculated that if you inhale 1 x 106 Bq, you will receive a thyroid dose of HT = 400 mSv (and weighted whole-body dose of 20 mSv).- Tritium. Tritium is a byproduct in nuclear reactors. Most important source (due to releases of tritiated water) of tritium in nuclear power plants stems from the boric acid, which is commonly used as a chemical shim to compensate an excess of initial reactivity. Note that, tritium emits low-energy beta particles with a short range in body tissues and, therefore, poses a risk to health as a result of internal exposure only following ingestion in drinking water or food, or inhalation or absorption through the skin. The tritium taken into the body is uniformly distributed among all soft tissues. According to the ICRP, a biological half-time of tritium is 10 days for HTO and 40 days for OBT (organically bound tritium) formed from HTO in the body of adults. As a result, for an intake of 1 x 109 Bq of tritium (HTO), an individual will get a whole-body dose of 20 mSv (equal to the intake of 1 x 106 Bq of 131I). While for PWRs tritium poses a minor risk to health, for heavy water reactors, it contributes significantly to collective dose of plant workers. Note that, “Air that is saturated with moderator water at 35°C can give 3 000 mSv/h of tritium to an unprotected worker (See also: J.U.Burnham. Radiation Protection). The best protection from tritium can be achieved using an air-supplied respirator. Tritium cartridge respirators protects workers only by a factor of 3. The only way to reduce the skin absorption is by wearing plastics. In PHWR power plants, workers must wear plastics for work in atmospheres containing more than 500 μSv/h.

Consistency in all Risks
Finally, it is all about the risks arising from exposure to ionizing radiation and about the consistency in all risks of everyday life. In general, danger (also risk or peril) is the possibility of something bad happening. A situation in which there is a risk of something bad happening, is called dangerous, risky or perilous. Yes, the term ionizing radiation sounds very dangerous, but how exactly dangerous radiation is?
Humans are often inconsistent in our treatment of perceived risks. Even though two situations may have similar risks, people will find one situation permissible and another unjustifiably dangerous. For radiation risks, doses to the public must be kept under 1 mSv/year. Even for very conservative case of linear non-threshold assumption, one millisievert represents a 0.0055% chance of some detrimental health effects. Two points:
- In our opinion, this is an acceptable risk. Note that, annual doses from natural background radiation in on average about 3.7 mSv/year (10 µSv = average daily dose received from natural background).
- Moreover, problem of this model is that it neglects a number of defence biological processes that may be crucial at low doses. The research during the last two decades is very interesting and shows that small doses of radiation given at a low dose rate stimulate the defense mechanisms.
Annually received dose of 1 mSv causes very conservatively about 0.0055% chance of some detrimental health effects. In April 2012, a year after the Fukushima accident, cleanup efforts are supposed to be happening wherever the radiation dose exceeds government regulations. Entire towns are still off limits because the annual dose from the ground is projected to be greater than 50 mSv or even 20 mSv, leaving many people in the area homeless and jobless. But did anyone take into account health effects of this evacuation. The consequences of low-level radiation are often more psychological than radiological. Forced evacuation from a radiological or nuclear accident may lead to social isolation, anxiety, depression, psychosomatic medical problems, reckless behavior, even suicide. Such was the outcome of the 1986 Chernobyl nuclear disaster in Ukraine. A comprehensive 2005 study concluded that “the mental health impact of Chernobyl is the largest public health problem unleashed by the accident to date”. But what if the threshold model is true, and doses of up to 100 mSv/yr actually result in no detectable health risks? This would mean that people are being unnecessarily kept away and prevented from working on their farms for negligible health effects. Recall that the annual dose in some parts of Araxa, Brazil is higher than 20 mSv while the average dose examined in the three-country nuclear worker studies was 30-40 mSv/yr, and that these studies found no significant increase in solid cancers or leukemias from those doses.
Another point of view can be obtained when we will consider all risks of everyday life. What about risks, which arise from transportation. Nearly 1.25 million people die in road crashes each year, on average 3,287 deaths a day. Road crashes are the leading cause of death among young people ages 15-29, and the second leading cause of death worldwide among young people ages 5-14. On a road, people don’t realize the kinetic energy of a car. So why we do not stop driving cars? Yes, transportation is today essential, but so are the peaceful uses of radiation. And what about smoking cigarettes? Cigarettes contain also polonium-210, originating from the decay products of radon, which stick to tobacco leaves. Polonium-210 emits a 5.3 MeV alpha particle, which provides most of equivalent dose. Heavy smoking results in a dose of 160 mSv/year to localized spots at the bifurcations of segmental bronchi in the lungs from the decay of polonium-210. This dose is not readily comparable to the radiation protection limits, since the latter deal with whole body doses, while the dose from smoking is delivered to a very small portion of the body.
Finally, we would like to discuss a very interesting fact. It is generally known, the increasing use of nuclear power and electricity generation using nuclear reactors will lead to a small but increasing radiation dose to the general public. But it is not generally known, power generation from coal also creates additional exposures, and, what is more interesting, while exposure levels are very low, the coal cycle contributes more than half of the total radiation dose to the global population from electricity generation. The nuclear fuel cycle contributes less than one-fifth of this. The collective dose, which are defined as the sum of all individual effective doses in a group of people over the time period or during the operation being considered due to ionizing radiation, is:
- 670-1400 man Sv for coal cycle, depending on the age of the power plant,
- 130 man Sv for nuclear fuel cycle,
- 5-160 man Sv for geothermal power,
- 55 man Sv for natural gas
- 03 man Sv for oil
Yes, these results should be seen from the perspective of the share of each technology in worldwide electricity production. Since 40 per cent of the world’s energy was produced by the coal cycle in 2010, and 13 per cent by nuclear, the normalized collective dose will be about the same:
- 7 – 1.4 man Sv/GW.a (man sievert per gigawatt year) for coal cycle
- 43 man Sv/GW.a (man sievert per gigawatt year) for nuclear fuel cycle
Special Reference: Sources and effects of ionizing radiation, UNSCEAR 2016 – Annex B. New York, 2017. ISBN: 978-92-1-142316-7.
We hope, this article, Danger of Ionizing Radiation – How Dangerous is Radiation, helps you. If so, give us a like in the sidebar. Main purpose of this website is to help the public to learn some interesting and important information about radiation and dosimeters.